
Shingles

-
- 20%. people have shingles at least once in their lifetime, and the incidence is rising.
- Varicella zoster virus can cause two different diseases: chickenpox and shingles.
- When a person gets chickenpox, the virus continues to live in the body (in the nerve nodes) without causing any symptoms, but when it becomes active it can cause herpes zoster.
- If you have never had chickenpox and have not been vaccinated against it, it is possible to get chickenpox from a person with shingles through direct contact with the rash or through inhalation of Varicella zoster virus.
- Approximately 1-6% of people develop recurrent shingles.
- Shingles should be distinguished from herpes zoster, rosacea, acute eczema, and the disseminated form from chickenpox.
Risk groups
-
- Shingles can affect people of all ages, but is most common in people over 50
- It is also more common in people of all ages, with weak immune systems (e.g. Oncology patients; patients with chronic, autoimmune diseases (rheumatoid arthritis, scarlet fever, etc.) – who are treated with systemic steroids, tumour necrosis factor (TNF)-alpha inhibitors, sphingosine-1-phosphate (S1P) receptor inhibitors, Janus kinase (JAK) inhibitors.
- People living with HIV and AIDS.


-
- A person with chickenpox, less commonly shingles
- Varicella zoster virus is transmitted by droplets in the air or by contact (touching the rash).
- Children can get chickenpox from a person with shingles, and vice versa
Provocative factors
-
- older age (>50 years)
- colds
- stress
- infections
- Injuries
- contact with a person with chickenpox or shingles
- UV rays
Localisation
-
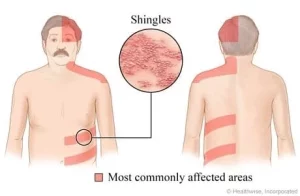
- 50% are intercostal (nn. intercostales, n. thoracicus) nerves in the thoracic and dorsal regions.
- 20% n.trigeminus; n.VII and n.VIII in the face.
- Less common are segments of the neck, lumbar spine and sacrum.
- In immunosuppression, may spread outside the segment to be anaesthetised

The clinical picture depends on the patient’s age and health status, and the affected area (dermatome). A dermatome is an area of skin innervated by a single spinal nerve.
-
- 3-5 d. general malaise, fatigue, fever, pain and burning in the area of the future rash before the skin is rubbed;
- Reddish spots-painful unilateral erythema (redness) – grouped papules, vesicles with clear fluid (12-24 hours) following the course of a nerve;
- Pimples – scabs (7-12 days)
- In severe cases: bloody-serous, gangrenous rashes
- Burning, pain, itching
Complications
-
- Skin: secondary bacterial infection may be present, with scarring during healing;
- Eyes: conjunctivitis, episcleritis, uveitis, keratitis, iridocyclitis (glaucoma), chorioretinitis (AIDS), retrobulbar neuritis, vasculitis, optic nerve atrophy. Herpes zoster ophthalmicus – lesion r. ophtalmicus n. Trigemini, vesicles appearing on one side of the eyelids and nose, affecting the cornea.
- Nervous system: encephalitis, meningitis, granulomatous arteritis, segmental paresis, N. facialis paresis, auditory nerve damage; postherpetic neuralgia is a very common complication. Pain without rashes, lasting for months or years. Hypo- or hyperaesthesia may be present and often requires medical treatment. a neurologist or pain medicine doctor for advice on pain relief.
- Internal organs: pneumonia, oesophagitis, myocarditis, enterocolitis, pancreatitis, arthritis.
Diagnostics
-
- Diagnosis is usually made by questioning and physical examination
- Laboratory tests can be used to confirm a definitive diagnosis if necessary:
-
- Polymerase chain reaction (PCR)
- Virological testing – growing the virus in infected cell cultures
- Direct immunofluorescence – to detect Varicella-zoster virus antigen
- Serological tests – IgM and IgG (Anti Varicella Zoster IgG and IgM)
- The material for testing is taken from the rash (vesicles).
-


Treatment recommendations
At the first sign of the disease, it is recommended to consult a doctor immediately. Do not self-treat, but consult your family doctor or a dermatovenereologist who will draw up the most appropriate treatment plan for you – this is the only way to avoid complications.
-
-
- Antiviral treatment is effective in reducing pain and symptom duration if started within 72 hours from the start of symptoms.
- More than 72 hours later the medicine can be given if new rashes appear.
- Do not rub, scratch or disinfect rashes to prevent them from growing
- Antiviral treatment is not indicated if the rashes are covered with scabs
- Other measures: rest, pain relief (cold, antiviral ointments, local steroids, emollients (creams, lotions, ointments – from the pharmacy), antiseptics, antibiotics in case of a secondary bacterial infection, B vitamins).
-
- In postherpetic neuralgia, it is important to:
-
- early antiviral treatment
- use of local anaesthetic
- a neurologist’s advice on how to relieve the pain (medications: non-steroidal anti-inflammatory drugs (NSAIDs), although usually not very effective, tricyclic antidepressants, antiepileptic drugs; non-medications: transcutaneous electrical nerve stimulation or acupuncture, injections into the affected areas).
-
Sick leave
-
- If the rash is on your face, don’t return to work until the scab has formed (~7-10 days)
- If the rash is in an area that you can cover (e.g. with a gauze bandage or clothes), you can return to work when you feel well.
- If you work in a healthcare facility (e.g. hospital, medical centre, nursing home), check with your doctor when it is safe to return to work.
Prevention
-
- Vaccination against Varicella zoster virus is recommended;
- Getting vaccinated can reduce your chances of developing shingles and postherpetic neuralgia
- The vaccination is recommended for adults over 50 years of age, but younger people can also be vaccinated, especially if their immune system is weaker than usual.

1. Harbecke R; cohen J I. Oxman M N. Herpes zoster vaccines. The Journal of infectious diseases. 2021; 224.Supplement_4: S429-S442.
2. Koshy, E., Mengting L., Kumar H., Jianbo W. Epidemiology, treatment and prevention of herpes zoster: A comprehensive review.
Indian Journal of Dermatology, Venereology and Leprology
. 2018;
84
(3).
3. Saguil A, Kane S F, Mercado M G, Lauters R. Herpes zoster and postherpetic neuralgia: prevention and management. American family physician, 2017; 96.10: 656-663.

Adult acne. Is acne just a teenage disease?
Adult acne. Is acne just a teenage disease? Acne is an inflammatory skin disease that has traditionally been considered a disease...

Rosacea
RosaceaA flush on the cheeks is not just for embarrassing situations or when you see someone dear to you a human being? Do you...

Seborrhoeic dermatitis
Bothered by scalp flaking and itching? You may have seborrhoeic dermatitisSeborrhoeic dermatitis is a common inflammatory skin...
iDerma
MB iDerma
Fabijoniškės g. 99, Vilnius
+370 670 70 822
[email protected]